
MAP IN CROHN'S DISEASE (AGAIN)
2023-06-11 15:52:58A team of 11 Portuguese scientists and one MAP expert from the UK have yet again demonstrated live MAP in the blood of Crohn’s Disease (CD) patients and confirmed the association of MAP and CD. In addition, they showed that MAP was far more common in CD patients than was Escherichia coli bacteria with adherence/invasive ability (AIEC). This type of E. coli has been suggested by some scientists to be a causal agent for CD. This work was published June 7 in the journal Microoganisms.
ABSTRACT
Pathobionts, particularly Mycobacterium avium subsp. paratuberculosis (MAP) and Escherichia coli isolates with adherence/invasive ability (AIEC) have been associated with inflammatory bowel disease (IBD), particularly Crohn’s disease (CD). This study aimed to evaluate the frequency of viable MAP and AIEC in a cohort of IBD patients. As such, MAP and E. coli cultures were established from faecal and blood samples (with a total n = 62 for each) of patients with CD (n = 18), ulcerative colitis (UC, n = 15), or liver cirrhosis (n = 7), as well as from healthy controls (HC, n = 22). Presumptive positive cultures were tested by polymerase chain reaction (PCR), for a positive confirmation of MAP or E. coli identity. E. coli-confirmed isolates were then tested for AIEC identity using adherence and invasion assays in the epithelial cell line of Caco-2 and survival and replication assays in the macrophage cell line of J774. MAP sub-culture and genome sequencing were also performed. MAP was more frequently cultured from the blood and faecal samples of patients with CD and cirrhosis. E. coli presumptive colonies were isolated from the faecal samples of most individuals, in contrast to what was registered for the blood samples. Additionally, from the confirmed E. coli isolates, only three had an AIEC-like phenotype (i.e., one CD patient and two UC patients). This study confirmed the association between MAP and CD; however, it did not find a strong association between the presence of AIEC and CD. It may be hypothesized that the presence of viable MAP in the bloodstream of CD patients contributes to disease reactivation.
COMMENTS
This study adds to the body of literature on the association of MAP and CD and strengthens the argument that MAP is a zoonotic pathogen, i.e., one transmissible from animals to humans. For more about MAP as a zoonotic pathogen and its link to Crohn’s Disease, see this page on our website where a long list of references on the subject is provided, with direct links to the original publications.
JD PATHOLOGY IN GOATS
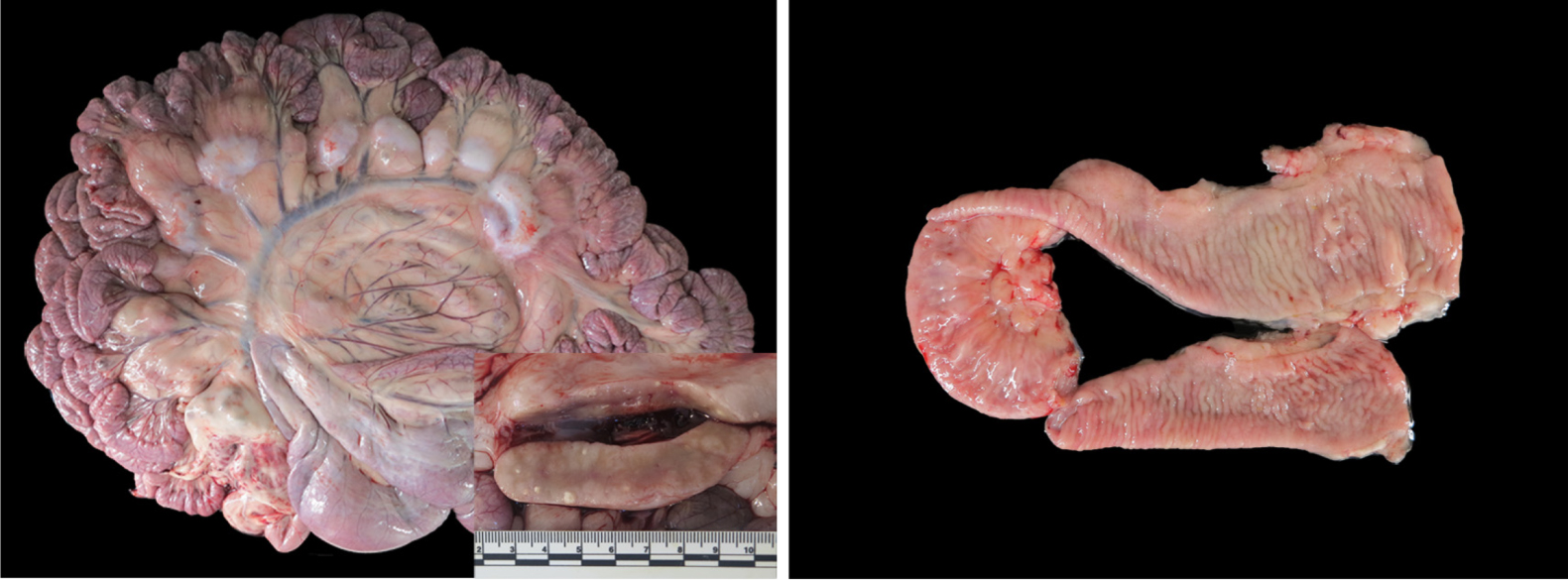
2023-05-27 15:20:53E. Stefanova and nine colleagues in Spain have published an article on Johne’s disease pathology in goats. They contrast the pathology found in non-vaccinated goats and goats that have been vaccinated with a commercial heat-inactivated vaccine for Johne’s disease. They also describe lesions caused by bronchopneumonia and caseous lymphadenitis (CLA) plus pathology caused by assorted other disease problems. The pictures of gross pathology are particularly good. Mesenteric lymph nodes were a the most valuable tissue to sample for detection of MAP infections in goats by histopathology. This Open Access article was published in the journal Animals on May 19, 2023.
SUMMARY
Paratuberculosis (PTB), also called Johne’s disease, is a well-known disease with considerable financial impact on the farm industry worldwide. Nevertheless, data regarding the assessment of naturally infected goat herds is limited. The present study describes in detail the observed gross and histological lesions detected in 39 necropsies of goats (15 vaccinated and 24 non-vaccinated) from herds with a confirmed history of PTB. PTB microscopic lesions of various grades were detected in all animals in target organs and the presence of the causative agent was confirmed using different laboratory tools. The main inflammatory findings affected the hemolymphatic, respiratory and gastrointestinal systems. The lesions were confirmed microscopically with lesser macroscopically visible alterations. Our result demonstrated that non-vaccinated animals presented more severe PTB intestinal lesions and had respiratory inflammation in all age groups studied. Those also presented a higher prevalence of ileocecal valve PTB lesions. Gastrointestinal non-PTB lesions were detected in higher number in non-vaccinated goats. Thus, histology is a powerful tool for herd diagnosis and assessment. Mainly inflammatory lesions of the respiratory and gastrointestinal tract were detected in the studied PTB-affected herds. Additionally, vaccination against PTB could play a key role in the reduction of lung and gastrointestinal inflammatory processes present in the herd.
COMMENTS
The Gudair® vaccine used in this study is a commercial heat-inactivated vaccine containing 2.5 mg/mL of MAP strain 316 F with mineral oil adjuvant (CZ Vaccines S.A., Spain). In Spain, it is primarily used in sheep and goats. This vaccine is not licensed for use in the United States.
CONTROL PROGRAMS WORK!
2023-04-26 16:23:41 R. Scarpelli together with seven Italian colleagues reported on the success of the Voluntary National Control Plan and Guidelines developed by the Italian Ministry of Health in 2013 at controlling paratuberculosis in Italian dairy herds of varying sizes.
R. Scarpelli together with seven Italian colleagues reported on the success of the Voluntary National Control Plan and Guidelines developed by the Italian Ministry of Health in 2013 at controlling paratuberculosis in Italian dairy herds of varying sizes.
Their publication appears in the June 2023 issue of Preventive Veterinary Medicine.
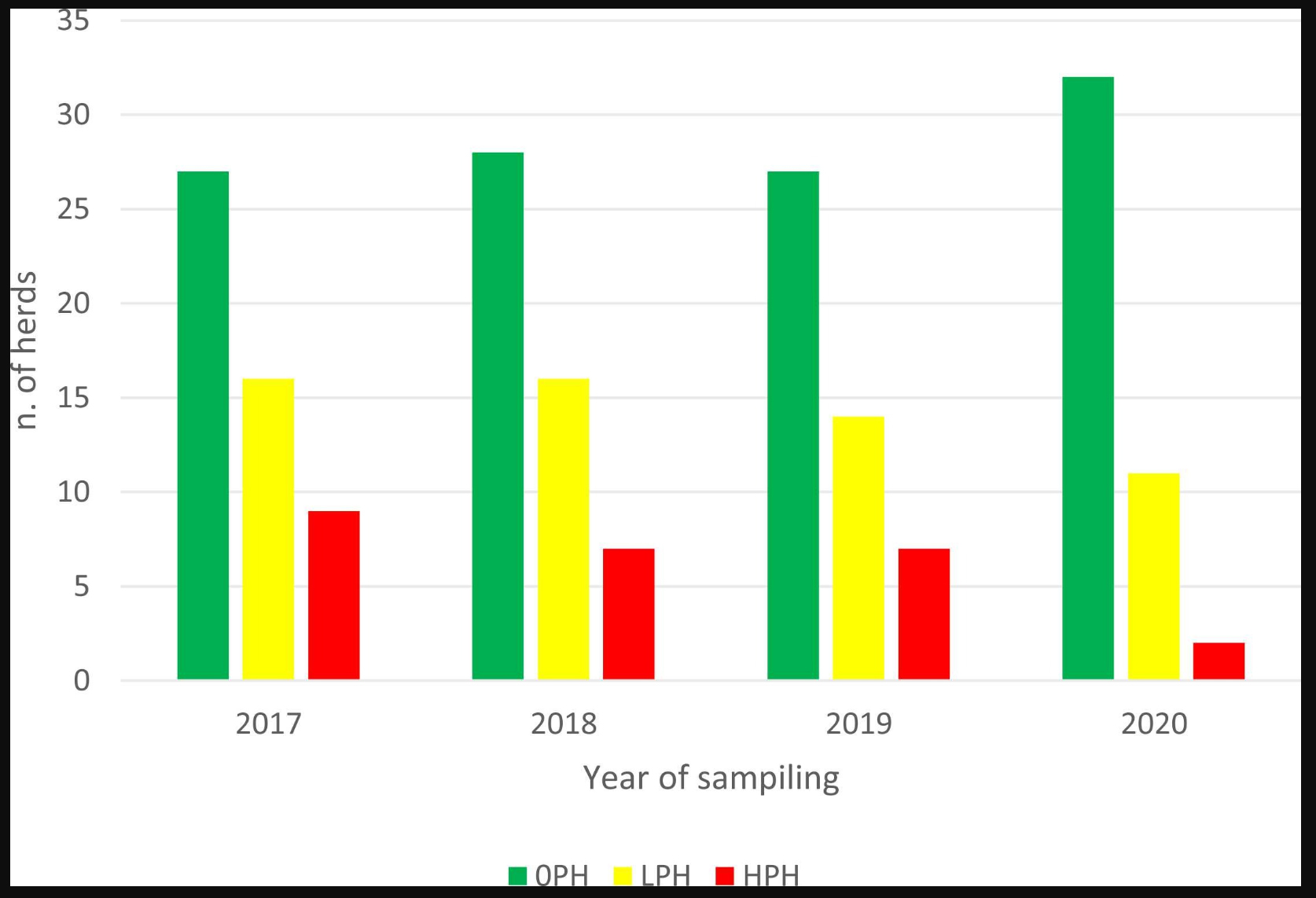
This graphic from their publication shows a steady rise in the number of ELISA negative herds (green bars), and a concomitant decrease in the number of herds with a low percentage of ELISA-positive animals (yellow bars) and number of herds with a higher percentage of ELISA-positive cows (red bars) over the time period of the study, 2017 to 2020. Interestingly, one farm that decided not to follow the proposed control program, but accepted to be sampled every year, showed an increasing rate of ELISA-positive cows (from 5.2% in 2017 to 7.6% in 2020).
ABSTRACT
Paratuberculosis is considered one of the most economically devastating infectious diseases of domestic livestock, and the most effective control strategy is a combination of ‘test-and-cull’ and on-farm biosecurity measures. In Italy, a Voluntary National Control Plan (VNCP) and guidelines have been introduced to reduce the impact of the disease, and farmers can voluntarily enroll in the control plan. The main aims of this study were: i) the description of the trend over a 4-year period on total, within-herd (WH) and between herd (BH) apparent seroprevalences observed in 64 dairy herds members of a mutual company located in Italy after the introduction of a proposed “Customized Control Plan” (CCP); ii) the evaluation of its effectiveness in terms of percentage of participating farms that decided to join the VNCP. Analyses on serum samples were performed with Enzyme-Linked ImmunoSorbent Assay (ELISA) method and revealed a general decrease in both total, WH and BH apparent seroprevalence. Total average apparent seroprevalence decreased from 2.39% in 2017 to 1% in 2020. Negative herds rose from 51.9% in 2017 to 71.1% in 2020, while farms with WH apparent seroprevalence >5% decreased from 17.3% in 2017 to 4.4% in 2020. BH apparent seroprevalence decreased from 51.2% in 2017 to 29.2% in 2020. Among the 52 out of 64 herds that accepted to continue the proposed CCP after the first year, 41 (78.8%) joined in 2020 the VNCP, that assessed the health ranking of the herds. The results provide evidence that a control plan based on a farm-specific strategy and a subsidized testing process can effectively reduce the impact of paratuberculosis in dairy herds, especially in convincing farmers to continue in paratuberculosis control by joining the VNCP, including them in a national context and increasing their awareness of the disease.
COMMENT
This study adds to the body of literature showing that paratuberculosis (Johne’s disease) in dairy cattle herds can be controlled using a cost-effective diagnostic test (ELISA) combined with herd management changes.
INTERNATIONAL PARATUBERCULOSIS SITUATION
2023-03-20 15:14:36The 7th and 8th IDF Paratuberculosis Fora took place on 26 May 2021 and 12 June 2022 respectively. The 7th event was virtual while the 8th Forum was held in conjunction with the International Colloquium on Paratuberculosis in Dublin, Ireland, and both were chaired by Dr. David Kelton (Chair of IDF Standing Committee on Animal Health and Welfare). The participants shared insights about the current situation and control measures of their respective countries on Mycobacterium avium subsp. paratuberculosis (M. paratuberculosis).
The Fora offered a unique opportunity for sharing past, present, and future perspectives on paratuberculosis (M. paratuberculosis, ParaTB) control, and served as a place for engaging in meaningful international discussion about how to address this globally important issue. The Fora highlighted the need for more investment in animal health, and opportunities for some harmonization and more research on factors affecting the disease progression. This publication contains a selection of eight papers, all of which were presented by program representatives on the 7th or the 8th ParaTB Fora days.
The Proceedings are available for download FREE at the IDF website.
TESTING CALF ENVIRONMENTS FOR MAP BY PCR
2023-02-18 16:57:23N.L. Field and colleagues in Ireland have published their research correlating MAP detection rates in areas where dairy calves are housed and the risk assessment scores (RAMP) for the farm. The publication appears in the journal Animals 2023, 13, 669. https://doi.org/10.3390/ani13040669.

This is their summary (British spellings):
Transmission of Mycobacterium avium subspecies paratuberculosis (MAP) from infected adult cattle to susceptible calves occurs mainly through contamination of the calf environment, i.e., the calving pen and the pre-weaned calf rearing area, with adult faeces. Control programmes for Johne’s disease utilise a risk assessment and management plan (RAMP) to evaluate the risk of transmission of infection on a specific farm, however the assessment is limited by its subjective, point-in-time nature. The objective of this study was to evaluate a novel environmental sampling protocol for measurement of MAP contamination of the calf environment on infected farms. Across 28 infected farms, 46% had detectable MAP in the calf environment, with 21% of farms having detectable MAP in the pre-weaned calf area. There was no significant association found between the RAMP scores for each farm and the result of environmental testing for MAP, and there was a moderate correlation found between RAMP scores and the level of MAP contamination as quantified by PCR. We conclude that environmental sampling is a potentially useful tool to objectively measure transmission risk in the calf environment on farms, as a complement to the annual RAMP.
COMMENT
PCR has replaced culture as the most accurate, cost-effective, and quantitative method for MAP detection. It can be applied to a wide range of sample types including feces, fresh and formalinized tissues, and environmental samples. Commercially available kits provides for high reproducibility of results among laboratories. In the U.S. the laboratory proficiency assessment by USDA offers additional confidence in PCR tests for MAP. The results of the proficiency test create a list of USDA-approved laboratories available on this website. Not all labs will accept environmental samples. So, contact your veterinary diagnostic lab of choice to be sure before sending such samples.
HAPPY BIRTHDAY DR. JOHNE
2022-12-10 16:25:58 One-hundred eighty-three years ago, on December 10, 1839, Heinrich Albert Johne was born in Dresden, Germany. It seems fitting that Johnes.org celebrate, on this date, his lasting contribution to veterinary medicine.
One-hundred eighty-three years ago, on December 10, 1839, Heinrich Albert Johne was born in Dresden, Germany. It seems fitting that Johnes.org celebrate, on this date, his lasting contribution to veterinary medicine.
Below you will find the story of his discovery, a brief biography, a little about the pathogen name, and the story of how I found this photo.
How it all started.
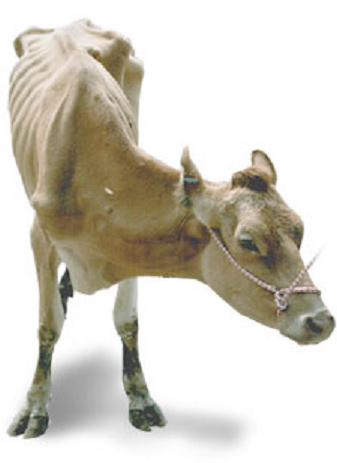 Dr. F. Harmes, a veterinarian in the Oldenburg region of Germany in 1895, had a client with a Guernsey cow that was doing poorly. Dr. Harmes’ preliminary diagnosis was intestinal tuberculosis (TB). TB in cattle was quite common in Germany then. But when he did the tuberculin skin test to confirm his diagnosis, the cow tested negative. So, the reason for the cow’s condition remained a mystery.
Dr. F. Harmes, a veterinarian in the Oldenburg region of Germany in 1895, had a client with a Guernsey cow that was doing poorly. Dr. Harmes’ preliminary diagnosis was intestinal tuberculosis (TB). TB in cattle was quite common in Germany then. But when he did the tuberculin skin test to confirm his diagnosis, the cow tested negative. So, the reason for the cow’s condition remained a mystery.
A few months later, the cow died. Curious as to what killed the cow, Dr. Harmes sent intestines and other tissues to the Pathology Unit at the veterinary school in Dresden. There the tissues were examined by Dr. Heinrich A. Johne, Professor of Pathology, and Dr. Langdon Frothingham, a visiting scientist from the Pathology Unit in Boston, Massachusetts.
 They observed that the small intestine was quite a bit thicker than expected and that lymph nodes near this thick intestine were enlarged. The photo at the right shows a normal intestine at the top and the intestine thickened due to Johne’s disease at the bottom. Lymphoid tissue, called Peyer’s Patches, are also quite prominent (the raised and slightly red tissue running long-ways down the center of the thickened intestine). Interestingly, Dalziel in 1913 saw the same kind of pathology when he removed a section of intestine from a person with Crohn’s disease remarking in his report that it resembled the cattle problem Dr. Johne had described.
They observed that the small intestine was quite a bit thicker than expected and that lymph nodes near this thick intestine were enlarged. The photo at the right shows a normal intestine at the top and the intestine thickened due to Johne’s disease at the bottom. Lymphoid tissue, called Peyer’s Patches, are also quite prominent (the raised and slightly red tissue running long-ways down the center of the thickened intestine). Interestingly, Dalziel in 1913 saw the same kind of pathology when he removed a section of intestine from a person with Crohn’s disease remarking in his report that it resembled the cattle problem Dr. Johne had described.
Using what at the time were newly developed histopathology techniques, parts of the intestine were “fixed” (pickled in formaldehyde), sliced into very thin sections, placed on a microscope slide, and stained with special dyes – known as an acid-fast stain - designed to help visualize bacteria of the type causing TB.
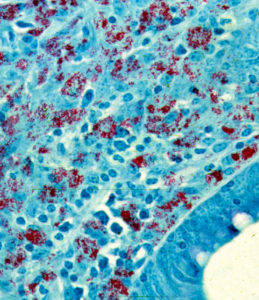
Under the microscope, Drs. Johne and Frothingham saw that the intestinal wall was filled with inflammatory cells of the kind to be expected in TB (macrophages and lymphocytes – the blue-colored stuff in the photo). In addition, they saw abundant red-staining bacteria (which microbiologists call acid-fast bacteria) throughout the inflamed tissues. Basically, it looked just like intestinal TB. But, when a sample of the fresh infected tissue containing the red-staining bacteria was injected into guinea pigs, it didn’t cause TB. This took place shortly after Louis Pasteur had devised the “germ theory” of disease and before techniques for growing bacteria in the laboratory were widely available. Inoculating animals, therefore, was a routine way of detecting infectious microbes such as those that cause TB, and guinea pigs are quite susceptible to tuberculosis. So, the diagnosis on this cow remained a mystery.
Drs. Johne and Frothingham concluded that the disease seen in the very sick Guernsey cow was caused by a bacterium other than the one normally causing TB in cattle, namely Mycobacterium bovis. They speculated that perhaps the pathology was due to a related bacterial pathogen such as the one causing TB in birds, aptly named Mycobacterium avium. Considering their subject’s gross pathology, microscopic pathology (histopathology) and animal inoculation findings, they proposed the name "pseudotuberculous enteritis" for the disease; a designation meaning inflammation of the intestine resembling intestinal TB but not actually the same as intestinal TB – somehow different. Soon after publication of their report, veterinarians began reporting outbreaks of this curious intestinal malady among dairy cows in Denmark, The Netherlands and elsewhere in continental Europe.
More on Dr. Johne.
H.A. Johne was the son of a veterinarian. Twenty years later, he became a veterinarian himself and held a practice for the next seven years. From 1866-1876, he acted as district veterinary inspector. He was then appointed to a lectureship at the veterinary school in Dresden. For a teacher of veterinary medicine, he lectured in an unusually wide range of subjects: embryology, histology, obstetrics, exterior, physical diagnostics. In 1879, he was appointed professor of pathological anatomy and of general pathology. Later he also lectured on parasitology and methodical zoology, and he also started classes in such a new branch of research as bacteriology.
As a scientist, he concerned himself with tuberculosis, anthrax, rabies, glanders, actinomycosis, bothryomycosis among others. As a writer he left a wide literary production. His books were printed in a dozen editions. For many years he also edited “Zeitschrift tor Tiermedizin”, and acted as co-editor of “Rundschau auf dem Gebiet der Fleischbeschau”. In 1887, he visited Denmark, where he was nominated honorary member of the Danish Association of Veterinarians and decorated with the Order of Knight of the Dannebrog.
He was often guest of Professor B. Bang and his family, the flat of Bangs' is today the Veterinary History Museum, established in 1973 at the Royal Veterinary and Agricultural University in Copenhagen. His motto was: Duty Above All. With the distinguished array of titles: Geheim-Medizinalrat, Professor, Dr. med., Dr. med.vet.h.c. and Dr. phil., Heinrich Albert Johne retired in 1904, respected and honored by his many students and by foreign veterinary schools and societies. He died in 1910.
MAP
In 1912, in one of those curious discoveries by serendipity, Twort and Ingram discovered how to grow the cause of Johne’s disease in the laboratory and named this bacterial pathogen Mycobacterium enteritidis chronicae pseudotuberculosae bovis johne. Time and technology led to name changes and the cause of Johne’s disease is today known as Mycobacterium avium subspecies paratuberculosis or simply MAP. Johne’s disease, also called paratuberculosis, is now a disease of major global importance.
Dr. Johne photo credit
I found the photo of Dr. Johne was hanging in halls of the State Veterinary Serum Institute when I was on sabbatical working with Dr. J.B. Jørgensen at the State Veterinary Serum Laboratory, Copenhagen, Denmark. Together we were comparing new methods for culturing MAP from clinical samples. On my departure, Dr. Jørgensen gifted me a copy of this photo which hangs in my office and also appears on the Wikipedia page about Dr. Johne.
PS
For more historical events and people important to understanding of Johne’s disease visit our history timeline.
CROHN'S DISEASE
2022-08-15 14:48:10MAP has long been associated with Crohn’s disease and many patients have benefited from anti-MAP antibiotic therapy. You can read one such story where a veterinarian was fully cured of Crohn’s disease by anti-MAP antibiotic therapy here.
 Dr. Marcel Behr, Professor of Medicine at McGill University and Associate Director of the Infectious Diseases and Immunity in Global Health Program at the Research Institute of the McGill University Health Centre conducted an interview on research connecting Crohn’s disease to MAP. To me, it is one of the most thoughtful, objective assessments of the state of research on the MAP=CD hypothesis I have ever witnessed. The interview covers every aspect of the research on this association in a lucid, straight forward discussion of this controversial topic.
Dr. Marcel Behr, Professor of Medicine at McGill University and Associate Director of the Infectious Diseases and Immunity in Global Health Program at the Research Institute of the McGill University Health Centre conducted an interview on research connecting Crohn’s disease to MAP. To me, it is one of the most thoughtful, objective assessments of the state of research on the MAP=CD hypothesis I have ever witnessed. The interview covers every aspect of the research on this association in a lucid, straight forward discussion of this controversial topic.
The interview is on You Tube. I appeared online August 13, 2022. It is 57 minutes long and, due to its technical nature, is probably best appreciated by physicians, veterinarians, Crohn’s disease patients, and people who follow this line of research.
Those wanting more background on this subject should visit the page on this site titled Zoonotic Potential where a synopsis of the subject is presented together with a long list of the primary research papers related to the subject and direct links to the full publications.
MAP VS HUMANS
2022-06-03 15:06:27Dr. C.T. Dow and Ms Briana L. Alverez from the University of Wisconsin-Madison have published a review article in EcoHealth titled: Mycobacterium paratuberculosis zoonosis is a One Health emergency. The article is Open Access (free to everyone), well-written, succinct (7 pages plus references) and well-researched with 113 literature citations.
ABSTRACT
A singular pathogen has been killing animals, contaminating food and causing an array of human diseases. Mycobacterium avium subspecies paratuberculosis (MAP) is the cause of a fatal enteric infectious disease called Johne’s (Yo’-nees), a disorder mostly studied in ruminant animals. MAP is globally impacting animal health and imparting significant economic burden to animal agriculture. Confounding the management of Johne’s disease is that animals are typically infected as calves and while commonly not manifesting clinical disease for years, they shed MAP in their milk and feces in the interval. This has resulted in a ‘‘don’t test, don’t tell’’ scenario for the industry resulting in greater prevalence of Johne’s disease; furthermore, because MAP survives pasteurization, the contaminated food supply provides a source of exposure to humans. Indeed, greater than 90% of dairy herds in the US have MAP-infected animals within the herd. The same bacterium, MAP, is the putative cause of Crohn’s disease in humans. Countries historically isolated from importing/exporting ruminant animals and free of Johne’s disease subsequently acquired the disease as a consequence of opening trade with what proved to be infected animals. Crohn’s disease in those populations became a lagging indicator of MAP infection. Moreover, MAP is associated with an increasingly long list of human diseases.
Despite MAP scientists entreating regulatory agencies to designate MAP a ‘‘zoonotic agent,’’ it has not been forthcoming. One Health is a global endeavor applying an integrative health initiative that includes the environment, animals and humans; One Health asserts that stressors affecting one affects all three. Recognizing the impact MAP has on animal and human health as well as on the environment, it is time for One Health, as well as other global regulatory agencies, to recognize that MAP is causing an insidious slow-motion tsunami of zoonosis and implement public health mitigation.
COMMENT
The discussion section of this publication summarizes the situation best and so it is quoted here:
The incidence of T1D in children is increasing worldwide (Hummel et al. 2012) as is the incidence of Crohn’s disease (Torres et al. 2017). Both the principle of parsimony and Koch’s postulates support inculpation of MAP as a cause of Crohn’s disease. Regardless of the relative strength one might assign to the MAP/Crohn’s association, this article enumerates other MAP-associated diseases and the increasing medical literature supporting it (Ekundayo and Okoh 2020). The combined weight of these disease associations should incite a call to action by regulatory agencies to invoke the precautionary principle with regard to consumption of MAP-contaminated food in at-risk individuals. In spite of public health implications, contamination of milk and dairy products with MAP is not currently restricted. We view the management of public health risk due to MAP as an increasingly important policy issue. With mounting global recognition of the impact MAP has upon the health of the environment, animals and humans, One Health is well positioned at that nexus (Fig. 1). One Health is in a unique position to elevate the discussion to mitigate this emerged yet neglected zoonotic pathogen: Mycobacterium avium subspecies paratuberculosis.
IRISH JD REVIEW
2022-05-26 15:07:56N. Field from the Animal and Bioscience Research Department, Teagasc, Moorepark Research Centre, Fermoy, Co. Cork, Ireland and colleagues have published an excellent Open Access article concerning Johne’s disease in the Irish Veterinary Journal. The article is succinct and comprehensive with 99 references cited. The pathogenesis of Johne’s disease is described briefly followed by an excellent summary comparing the accuracy of diagnostic tests for Johne’s disease both at the individual cow-level and herd-level using the latest research findings.

ABSTRACT
Johne’s disease is an infectious disease affecting cattle, other ruminants and non-ruminant wildlife worldwide, caused by Mycobacterium avium subspecies paratuberculosis (MAP). This review provides an up-to-date concise overview of the pathogenesis of MAP, the significance of Johne’s disease in cattle and the use of diagnostic testing at both animal and herd level in the context of seasonal pasture-based herds. While MAP can only replicate intracellularly, the bacterium is sufficiently robust to survive for months in the environment. Transmission of MAP is mostly via the faecal-oral route, however in-utero transmission in also possible. The bacteria evade the immune system by persisting in macrophages in the small intestine submucosa, with this latent stage of infection lasting, in most cases, for at least two years before bacterial shedding and clinical signs begin. The slowly progressive nature of MAP infection, poor performance of diagnostic tests and management systems that expose susceptible calves to infection make control of Johne’s disease challenging, particularly in seasonal calving herds. Testing of individual animals provides little assurance for farmers and vets due to the poor sensitivity and, in the case of ELISA, imperfect specificity of the available tests. Repeated herd-level testing is utilised by the IJCP to detect infected herds, identify high risk animals, and provide increasing confidence that test-negative herds are free of infection. The IJCP aims to control the spread of Johne’s disease in cattle in Ireland, in order to protect non-infected herds, limit the economic and animal health impact of the disease, improve calf health and reassure markets of Johne’s disease control in Ireland.
COMMENT
Ireland is the latest country to implement a national Johne’s disease control program and their scientists are concurrently generating research of practical importance to help drive the program. This publication is just one of many excellent products in recent years. Read more about the Irish program here.
DUBLIN MEETING ON MAP
2022-05-05 15:21:20The 15th International Colloquium on Paratuberculosis (15-ICP) will be held in Dublin Ireland, June 12-16, 2022.
To date, there are 182 registrants, and it is looking to be a very enjoyable conference. If you haven’t registered yet it’s not too late. The organizers are delighted with the number of abstracts submitted and have put together a strong scientific program. There are six plenary speakers, all experts from around the world, including Marcel Behr, Kumi De Silva, Frank Griffin, Marian Price Carter, Vivek Kapur and Herman Barkema.
There are six different sessions in the Scientific Program:
- Pathogenomics, Genotyping and MAP diversity (10 Oral Presentations)
- Control programs and Education (8 Oral Presentations)
- Diagnostics and detection (12 Oral Presentations)
- Host response and immunology (10 Oral Presentations)
- Epidemiology and Economics (10 Oral Presentations)
- Public Health and MAP in the environment (8 Oral Presentations)
A new feature at this colloquium is that before each poster session, five poster presenters will give a 2-minute pitch to encourage people to view their poster and discuss their research further. There are a total of 84 posters. The full program is available on the meeting website.
For details on travelling to Ireland please visit the Irish Government website.
There is also an interesting social program and you can anticipate many impromptu meetings, dinners and outings providing a chance meet leaders in MAP research personally. If you haven’t been before it is great opportunity to meet up with people working in the same field. There will be several social events targeted at graduate students, future MAP research leaders.
There is a Facebook page and a Twitter page. Details of places to visit when you come to Ireland will be included on these pages as well as Breaking News about the Colloquium.
COMMENT
This is the one and only international meeting focused on paratuberculosis (Johne’s disease) and the causative agent, MAP. It is always an exceptional meeting and a chance to meet and discuss this chronic, infectious, zoonotic pathogen of global importance with world experts.
« Previous 1 2 3 4 5 … 19 Next »