
WHY JD CONTROL FAILS
2021-03-19 01:00:02Swiss veterinarians followed Johne’s disease (JD) control programs in 7 beef cattle and 10 dairy herds over a 3-year period. They documented the degree to which owners adopted JD control recommendations and monitored the level of MAP infection in the herds primarily by fecal culture with some supplemental testing by ELISA and fecal PCR. This study was reported in the journal PLOS ONE and is Open Access.

ABSTRACT
Various measures have been advocated for the control of Johne’s disease (caused by Mycobacterium avium subsp. paratuberculosis, MAP) in different countries. Farmers’ compliance has been reported to be variable depending on disease prevalence and incentives to participate in control programs. After the prevalence of MAP shedding and risk factors for within-herd spread of MAP were assessed in 17 Swiss cattle herds (10 dairy and 7 beef), general and herd-specific recommendations were given to the farmers to reduce MAP transmission within the herd. Participation in the study and implementation of control measures were voluntary, no financial incentives were provided for the realization of control measures. After a 3-year period of monitored observation including biannual farm visits and discussion of the situation, the implementation of the recommended control measures and their effect on prevalence of MAP shedding were evaluated. Implementation of recommended general and farm-specific control measures was only partially realized. Neither the number of animals tested positive (before or during the study) nor the farmers’ knowledge about paratuberculosis were significantly associated with their compliance for the implementation of management changes. The apparent within-herd prevalence remained constant despite limited implementation of control measures, and no particular group of control measures was found to be associated with changes in prevalence. Farmers’ compliance for the implementation of control measures to reduce the impact of Johne’s disease in infected farms was very limited under Swiss farming conditions in the frame of voluntary participation in a research project. These results indicate that the losses associated with paratuberculosis in Swiss dairy and beef operations are not estimated to be high enough by the farmers to justify important efforts for control measures, and that incentives may be necessary to achieve efficient implementation of such measures.
CONCLUSIONS (from the publication)
The managers of infected Swiss dairy and beef herds were reluctant to implement control measures to minimize MAP spread in the frame of their voluntary participation in a research project conducted over a period of three years. Except for culling test-positive animals, implementation rates were low for most proposed measures, and some of those that were implemented at the beginning of the period of observation were discontinued in the course of the study. The farmers mostly implemented cheap and easy measures, while changes impacting farm structure or their routines more deeply, e.g. improving hygiene in the calving area or minimizing animal purchase, were rarely realized. The farmers did not observe relevant economic losses due to PTB in their herds and therefore did not expect an immediate reward for expenditures in time, efforts and money. These observations suggest that incentives for a consequent implementation of control measures should be included in future programs to increase the compliance of the managers of herds infected with PTB and thus improve the chances of successfully controlling the disease.
COMMENT
Despite many studies documenting the cost of Johne’s disease to both dairy and beef cattle operations, these costs are not readily apparent to producers. And, if these producers are expected to shoulder 100% of the cost of controlling Johne’s disease but perceive little financial benefit, programs will not likely succeed, as the Swiss study shows. When programs have broad industry support, and the meat and milk processors who buy raw products from producers pay a premium for products from herds that are successfully controlling Johne’s disease, control program costs are shared equitably, and programs are more likely to succeed. This is the basis of the most recent national programs underway in the UK and the Republic of Ireland. JD control program costs may be passed along to consumers in the form of slightly higher retail product prices, but consumers will benefit because JD control programs result in less MAP entering the food chain making the finished products safer to consume.
As a reminder:
- MAP is found in raw milk and meat.
- MAP survives pasteurization and is found in retail milk.
- MAP survives cooking unless the meat is cooked until it is “well-done”.
- MAP is routinely found in people with Crohn’s disease (a human disease resembling JD).
- People with Crohn’s disease clinically improve when treated with anti-MAP antibiotics; some have been fully cured.
MAP is likely a food-borne zoonotic pathogen affecting people worldwide. Just as for other zoonotic pathogens found in domestic animals, such as tuberculosis and brucellosis, control programs that benefit both animal and human health begin on the farm. This is fundamental to the One Health philosophy.
- Read more about MAP in food here.
- Read more about the zoonotic potential of MAP here or watch the video on this page.
JD IN BEEF CATTLE LECTURE
2021-03-12 13:10:55
Beef cattle producers and their herd veterinarians commonly ask:
- What is the best test to help control JD in beef cattle?
- What should I do with cattle that test ELISA-positive
- How can I avoid buying MAP-infected cattle?
- Which test should I use to certify my herd is free of Johne’s disease?
- What are my first steps in controlling Johne’s disease?
- Should I use the ELISA for JD on blood samples of PCR on fecal samples?
- Will JD control improve my farm profitability - what's the evidence?
- How common are national JD control programs and how to they work?
These and many more questions are addressed in a new 60-minute lecture titled “Johne’s Disease in Beef Cattle” now available on the Johnes.org website. This lecture is based on a a recent continuing education program for veterinarians. You will also find on this same web page lectures titled Johne’s disease in dairy cattle, parts-1 and 2” “Johne’s Disease in Goats” and “MAP is a Zoonotic Pathogen”.
NEW ASSAY FINDS MORE MAP IN MILK
2021-03-05 01:00:01Antonio Foddai and colleagues have developed a novel assay for detection of viable MAP in milk. The assay uses bacteriophages (viruses that attack bacterial cells) attached to magnetic beads to capture MAP in milk samples and then detect the presence of MAP by PCR. While these phages bind to both living and MAP cells, they only then infect and lyse live MAP. Thus, this assay only detects live MAP, just as do conventional culture methods. This new assay has higher diagnostic sensitivity and specificity than the most commonly used assay on milk today, the milk ELISA.
The article, published in the Journal of Dairy Science, is not Open Access, but is available for the next 40 days.
ABSTRACT
Bulk tank milk samples from 392 Northern Ireland dairy farms and individual milk from animals (n = 293) on 4 of these farms were tested by a novel phagomagnetic separation (PhMS)-quantitative (q)PCR assay able to detect and quantify viable Mycobacterium avium ssp. paratuberculosis (MAP), to demonstrate its potential utility as a milk surveillance tool. Viable MAP were detected in 26.5% of the bulk tank milks, with MAP contamination levels ranging from 1 to 8,432 MAP/50 mL of milk; less than 2% of farms had MAP contamination levels >100 MAP/50 mL in their bulk tank milk. Follow-up PhMS-qPCR testing of milk from individual animals on 4 farms that had the highest numbers of MAP in their bulk tank milks indicated that 17 to 24% of animals in each herd were shedding viable MAP in their milk. Mean MAP numbers detected ranged between 6.7 and 42.1 MAP/50 mL of milk. No significant correlation was observed between the detection of viable MAP in bulk or individual milks by PhMS-qPCR and parallel milk ELISA results, or between PhMS-qPCR results and any other milk recording results (somatic cell count, total bacterial count, % butterfat, or % protein). Viable MAP was detected by IS900 qPCR in 52 (85.2%) Pozzato broth cultures of 61 PhMS-qPCR-positive individual milks after 12 wk of incubation, suggesting few PhMS-qPCR results were false positives. The mean sensitivities of the PhMS-qPCR assay and milk ELISA applied to individual milks were estimated by Bayesian latent class analysis to be 0.7096 and 0.2665, respectively, and mean specificities were similar (0.9626 and 0.9509). Our findings clearly demonstrate that the novel PhMS-qPCR assay could be a useful milk surveillance tool for dairy processors, or a milk monitoring tool for Johne's disease control or milk quality assurance programs.
COMMENT
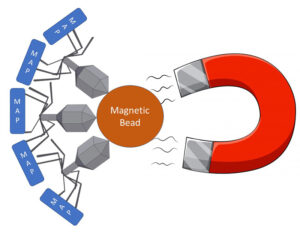
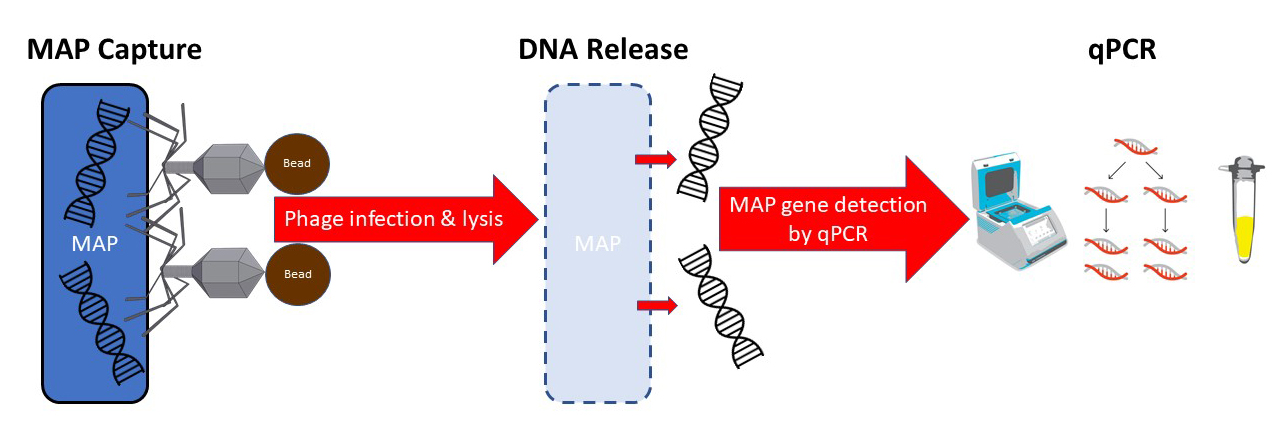
Phage-based assays for MAP have been described previously. This is the first time, however, that the phage has been linked to a magnetic bead allowing retrieval and concentration of MAP using magnets. In addition to binding to MAP, the phage then infects and lyses the live MAP bacterial cell, releasing its DNA allowing detection by qPCR technology. My schematic of the process appears below.
The head of the phage is linked to a magnetic bead. The tail of the phage binds to live mycobacteria. A magnet then pulls all of the beads+phage+MAP out of the sample.
After collecting the beads on a magnet, the phage then infects and lysis the live mycobacterial cells releasing their DNA. A qPCR specific for MAP then detects the pathogen. The phage-bead-magnet combination makes the assay very sensitive and the qPCR part of the assay makes it very MAP-specific.
Phage amplification assays for detection of mycobacterial infections were recently reviewed in the journal Microorganisms. This excellent 28 page Open Access article with 97 references provides a deeper understanding of phage-based mycobacterial detection technology but does not address this new twist: the use of phages to both capture and lyse the mycobacteria.
Actiphage is a commercial test, based on phage technology, for diagnosis of bovine tuberculosis and Johne's disease. Dr. Cath Rees (University of Nottingham) will be presenting a talk “Use of Actiphage to improve our understanding of mycobacterial diseases” on the 23rd March at 2pm as part of a virtual virology conference. Registration for the event is free.
The Wisconsin Connection
Fun factoid: Dr. Tom Brock, University of Wisconsin-Madison Professor, discovered a bacterium he named Thermus aquaticus, which grows at temperatures over 70 degrees C (158 degrees Fahrenheit) . Parts of its metabolic machinery, including the enzyme Taq polymerase, needed to assemble strands of DNA, tolerates boiling. In 1989, Science named Taq polymerase its first “molecule of the year,” because it enabled polymerase chain reaction (PCR), an essential tool for molecular biologists. Today's #1 test for COVID also depends on PCR.
The world owes a big "thank you" to Dr. Tom Brock.
DETECTION OF MAP-INFECTED DAIRY HERDS
2021-02-25 01:00:58![]() Vera Fichtelova and colleagues from the Veterinary Research Institute, Brno, Czech Republic published a study on the optimal method for detecting MAP-infected dairy herds using environmental fecal sampling. They found that fecal samples collected from the floor of the milking alleys (paths for cows to come into the milking area close to the entrance into the milking parlor holding pens) tested by qPCR (also known as real-time PCR) was a simple and effective method for detection of dairy herds with a significant MAP infection rate.
Vera Fichtelova and colleagues from the Veterinary Research Institute, Brno, Czech Republic published a study on the optimal method for detecting MAP-infected dairy herds using environmental fecal sampling. They found that fecal samples collected from the floor of the milking alleys (paths for cows to come into the milking area close to the entrance into the milking parlor holding pens) tested by qPCR (also known as real-time PCR) was a simple and effective method for detection of dairy herds with a significant MAP infection rate.
ABSTRACT
The objective of the present study was to evaluate the suitability of environmental sampling to screen Czech dairy herds to detect Mycobacterium avium ssp. paratuberculosis (MAP) and to find the most convenient location for the MAP detection in the lactating cow area. Environmental samples (ES, n = 72) from milking parlour holding pens (n = 19), milking alleyways (n = 19) and free-stall alleyways (n = 34) from 19 herds were simultaneously tested to detect MAP by a quantitative PCR (qPCR) and bacterial culture. Eight and thirteen samples from the milking parlour holding pens, twelve and eleven samples from the milking alleyways and eleven and eighteen samples from the free-stall alleyways were qPCR and culture positive, respectively. A 4.6 times higher probability of being culture positive than qPCR positive was detected for the assessable MAP detection results from the free-stall alleyways [P = 0.008 6, odds ratio (OR) = 4.572 8)] and no association was found between the results from the milking parlour holding pens (P = 0.191 4) and the milking alleyways (P > 0.999 9) and the diagnostic method used. The percentage of qPCR-positive samples in the tested locations was detected for the milking alleyways (63.2%), free-stall alleyways and milking parlour holding pens. The herd infectious status was in agreement with 16 (84.2%), 14 (73.7%) and 12 (63.2%) qPCR results from the milking alleyways, free-stall alleyways (32.4%) and milking parlour holding pens (42.1%), respectively. No statistically significant differences were detected for these results (P = 0.396 1). MAP was detected by the qPCR and bacterial culture in all three locations where the ES were collected. We suggest an environmental sampling followed by MAP detection by qPCR as an easy-to-perform time-saving protocol for MAP screening in Czech dairy herds. Although the milking alleyways seem to be the most convenient location for the environmental sampling, this assumption was not statistically supported.
COMMENT
The first step toward Johne’s disease control in commercial dairy herds (herds in the business of selling milk, not breeding animals) is to establish which herds have a significant MAP infection rate. Environmental fecal samples tested by qPCR provides a rapid, low-cost methods for testing the whole dairy herd.
The environmental fecal sample methods described in the U.S. Uniform Program Standards for the Voluntary Bovine Johne’s Disease Control Program are much more difficult to perform. Page 33 of that document states: “From each dairy farm, collect two composite environmental fecal samples tested by an MAPDT (MAP detection test meaning culture of PCR) from each of the following locations on the farm: manure concentration areas (cow housing alleyways or gutters), manure storage areas (lagoons, piles, pits, or manure spreader), and another manure concentration area (sick cow pens or other cow alleyways and travel-ways). A total of six samples should be collected for submission to the diagnostic laboratory.”
The Czech system may allow more herds to be tested at less cost and therefore may be preferable to the U.S. system. However, the critical question is whether the herd-level sensitivity is comparable between the U.S. method and the newly described Czech system and also the comparative utility of the two methods. A testing system that is too onerous and therefore not used is not useful.
COST OF JD TO THE DAIRY INDUSTRY
2021-02-18 16:10:38Philip Rasmussen from the Department of Ecosystem and Public Health, University of Calgary, Calgary, AB, Canada, and colleagues have published a study on the economic losses due to Johne’s disease in dairy cattle. Their Open Access article was published online in the Journal of Dairy Science January 14, 2021.

ABSTRACT
Johne's disease (JD), or paratuberculosis, is an infectious inflammatory disorder of the intestines primarily associated with domestic and wild ruminants including dairy cattle. The disease, caused by an infection with Mycobacterium avium subspecies paratuberculosis (MAP) bacteria, burdens both animals and producers through reduced milk production, premature culling, and reduced salvage values among MAP-infected animals. The economic losses associated with these burdens have been measured before, but not across a comprehensive selection of major dairy-producing regions within a single methodological framework. This study uses a Markov chain Monte Carlo approach to estimate the annual losses per cow within MAP-infected herds and the total regional losses due to JD by simulating the spread and economic impact of the disease with region-specific economic variables. It was estimated that approximately 1% of gross milk revenue, equivalent to US$33 per cow, is lost annually in MAP-infected dairy herds, with those losses primarily driven by reduced production and being higher in regions characterized by above-average farm-gate milk prices and production per cow. An estimated US$198 million is lost due to JD in dairy cattle in the United States annually, US$75 million in Germany, US$56 million in France, US$54 million in New Zealand, and between US$17 million and US$28 million in Canada, one of the smallest dairy-producing regions modeled.
COMMENT
This paper is informative, international in scope, and has an excellent list of references that backup the cost estimates used in this economic modelling exercise.
JD IN DAIRY CATTLE LECTURES
2021-02-12 01:00:52Dairy producers and their herd veterinarians commonly ask:
- What is the best test to help control JD in dairy cattle?
- What should I do with cattle that test ELISA-positive?
- How can I avoid buying MAP-infected cattle?
- Which test should I use to certify my herd is free of Johne’s disease?
- What are my first steps in controlling Johne’s disease?
- Should I use the ELISA for JD on blood (serum) or milk samples?
- Will JD control improve my farm profitability - what's the evidence?
- How common are national JD control programs and how to they work?

These and many more questions are addressed in a new two-part lecture series titled “Johne’s Disease in Dairy Cattle part 1 and part 2” (40 minutes each) now available on this website. You will also find on this same web page lectures titled “Johne’s Disease in Goats” and “MAP is a Zoonotic Pathogen”.
JOHNE’S DISEASE IN SAUDI ARABIA
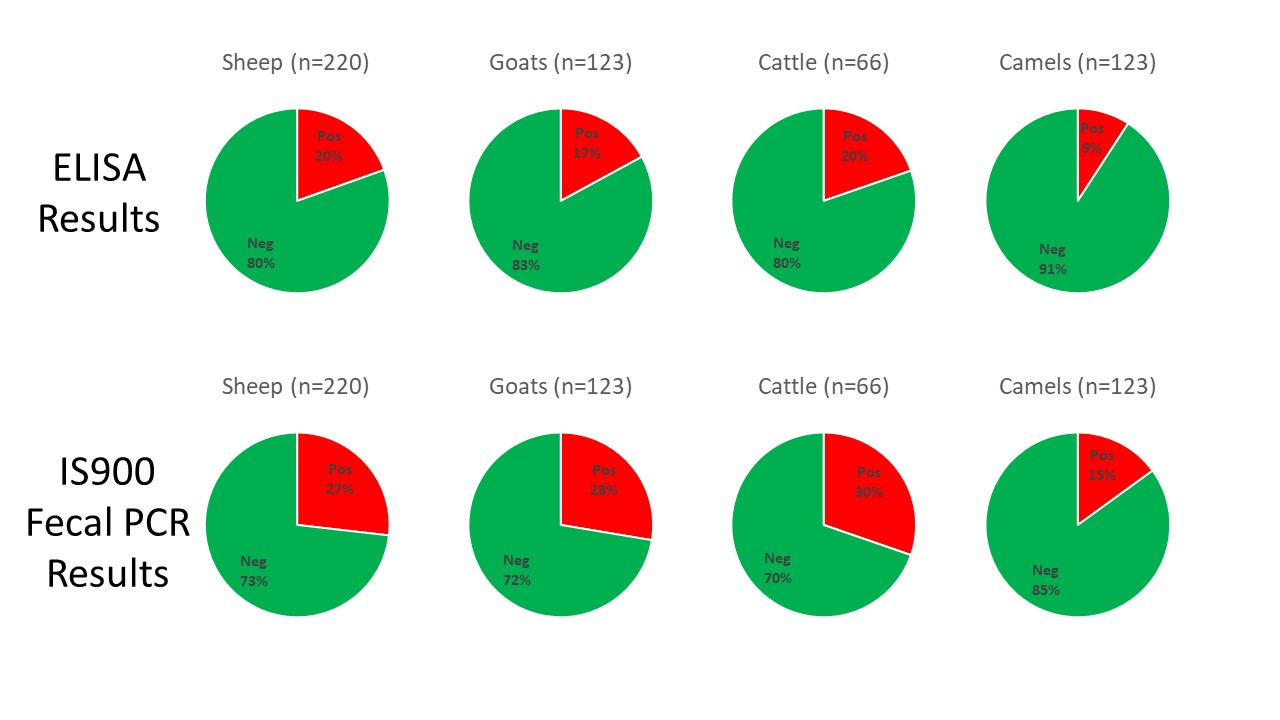
2021-02-06 01:00:06 An international team of researchers, led by Ibrahim Elsohaby, tested 31 herds of animals with prior histories of Johne’s disease in the Eastern Province in Saudi Arabia. The Eastern Province is the third most populous province in Saudi Arabia, with varying climatic conditions from semi-desert to desert. The Eastern Province shares the borders with five countries (Iraq, Kuwait, Oman, Qatar, and the United Arab Emirates), which may increase the risk of pathogen introduction to the country.
An international team of researchers, led by Ibrahim Elsohaby, tested 31 herds of animals with prior histories of Johne’s disease in the Eastern Province in Saudi Arabia. The Eastern Province is the third most populous province in Saudi Arabia, with varying climatic conditions from semi-desert to desert. The Eastern Province shares the borders with five countries (Iraq, Kuwait, Oman, Qatar, and the United Arab Emirates), which may increase the risk of pathogen introduction to the country.
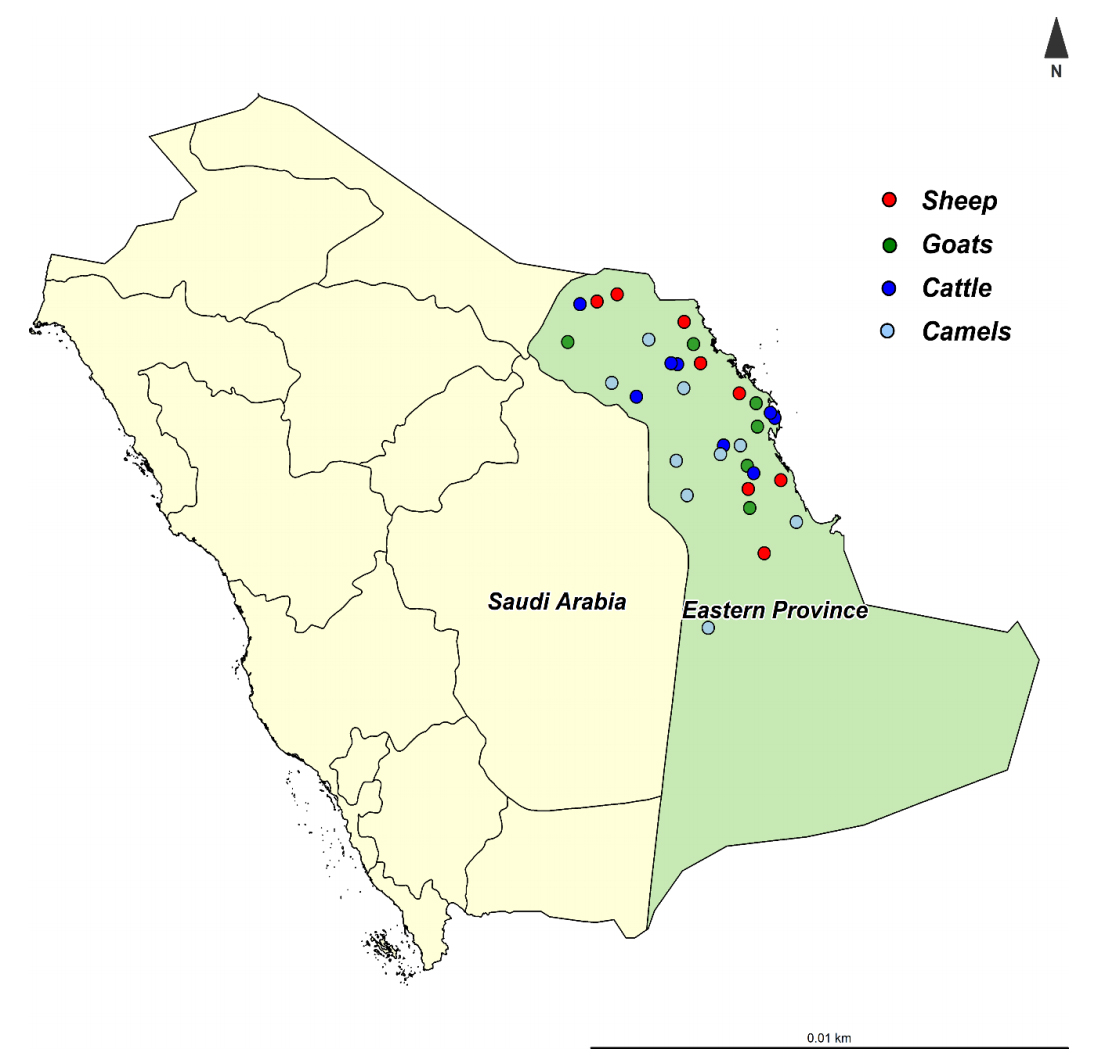
A total of 649 sheep, goats, cattle, and camels were tested by ELISA on serum samples and IS900 PCR on fecal samples. The study was reported this month in the journal Animals. The pie charts below were created to summarize the study findings. They reveal high infection rates among all four animals species and the higher diagnostic sensitivity of fecal PCR as compared to serum ELISAs. Interestingly, the S (sheep)-strain of MAP was more prevalent than the C (cattle)-strain.
Abstract
The objectives of the present study were to characterize Mycobacterium avium subsp. paratuberculosis (MAP) infection using serological and molecular tools and investigate the distribution and molecular characterization of MAP strains (cattle (C) and sheep (S) types) in sheep, goat, cattle, and camel herds in Eastern Province, Saudi Arabia. Serum and fecal samples were collected from all animals aged >2 years old in 31 herds (sheep = 8, goats = 6, cattle = 8 and camels = 9) from January to December 2019. Serum samples were tested by ELISA for the detection of MAP antibodies. Fecal samples were tested by PCR for the detection of MAP IS900 gene and the identification of MAP strains. MAP antibodies were detected in 19 (61.3%) herds. At the animal level, antibodies against MAP were detected in 43 (19.5%) sheep, 21 (17.1%) goats, 13 (19.7%) cattle and 22 (9.1%) camels. The IS900 gene of MAP was detected in 23 (74.2%) herds and was directly amplified from fecal samples of 59 (26.8%) sheep, 34 (27.6%) goats, 20 (30.3%) cattle and 36 (15.0%) camels. The S-type was the most prevalent MAP type identified in 15 herds, and all were identified as type-I, while the C-type was identified in only 8 herds. The IS900 sequences revealed genetic differences among the MAP isolates recovered from sheep, goats, cattle and camels. Results from the present study show that MAP was prevalent and confirm the distribution of different MAP strains in sheep, goat, cattle and camel herds in Eastern Province, Saudi Arabia.
This graphic from the publication shows an example of Johne's disease in goats.

Comment
Few reports on paratuberculosis in Saudi Arabia are available making this an important addition to the body of evidence that Johne’s disease is a global problem.
JOHNE’S DISEASE IN GOATS
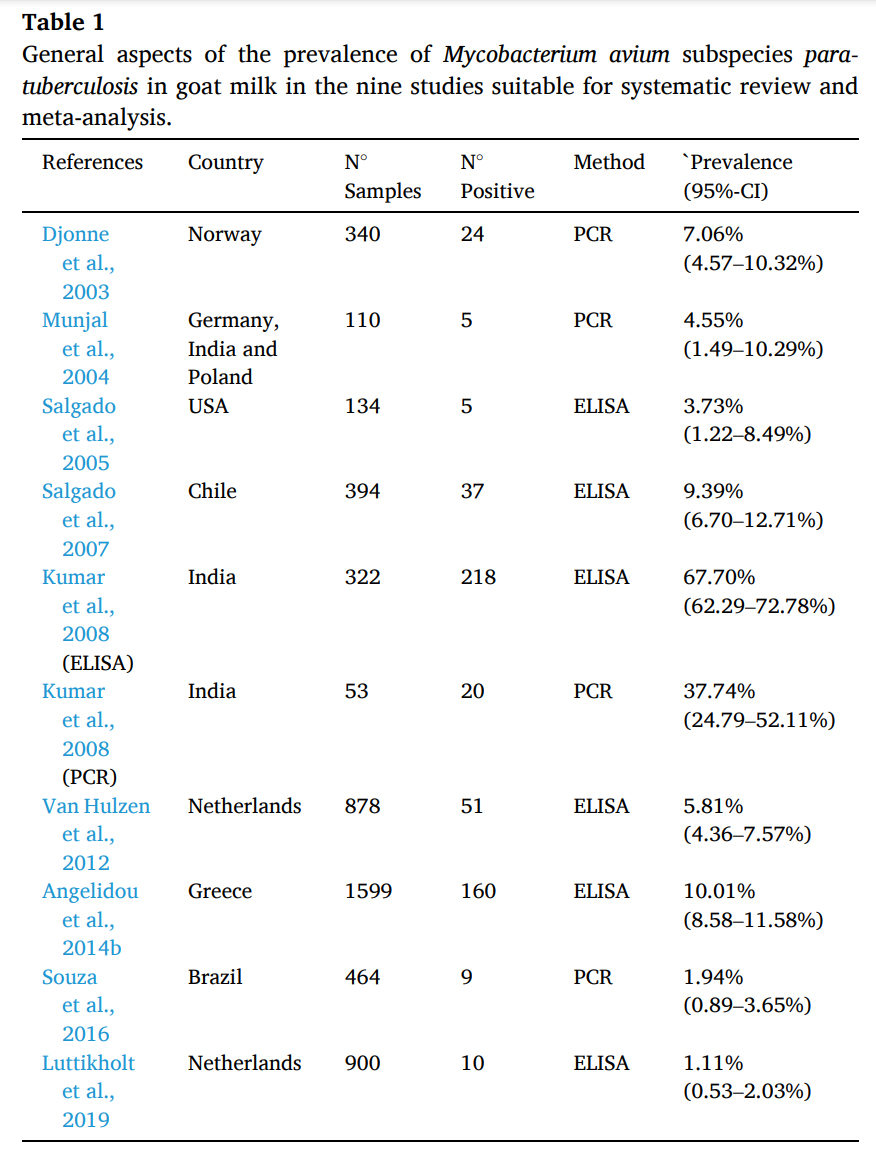
2021-01-28 01:00:46![]() João Paulo de Lacerda Roberto and 8 colleagues from the Federal University of Campina Grande, Post-Graduate Program in Animal Science and Health, Patos, PB, Brazil conducted a systematic review and meta-analysis on scientific articles concerning MAP in goats. They specifically examined reports on detection of antibody to MAP in goat milk and detection of MAP in goat milk by PCR methods. They found wide ranging herd-level prevalence estimates among countries as shown in their table below.
João Paulo de Lacerda Roberto and 8 colleagues from the Federal University of Campina Grande, Post-Graduate Program in Animal Science and Health, Patos, PB, Brazil conducted a systematic review and meta-analysis on scientific articles concerning MAP in goats. They specifically examined reports on detection of antibody to MAP in goat milk and detection of MAP in goat milk by PCR methods. They found wide ranging herd-level prevalence estimates among countries as shown in their table below.
Abstract
Paratuberculosis is an incurable infectious disease that affects several species, including goat (Capra hircus). The etiologic agent is Mycobacterium avium subspecies paratuberculosis (MAP) that has tropism for the intestine, causing anorexia, progressive weight loss and death. In goats, the main transmission route is the ingestion of water and food contaminated by infected feces. Affected animals also eliminate the agent through milk, with a potential biological risk to public health. Thus, the aim of this study was to conduct a research of the literature available in electronic media for a systematic review, followed by a meta-analysis of the results found on prevalence and diagnostic tests adopted in the detection of MAP antibodies and DNA in goat milk. The following search parameters were used: “Mycobacterium avium subsp. paratuberculosis” AND (goat OR small ruminant) AND (milk OR pasteurized milk). Strictly obeying pre-established criteria, 437 articles were selected from the respective electronic databases of scientific content: ScienceDirect (285), PubMed (68), Web of Science (60) and Scopus (24), of which nine papers were elected to the construction of the systematic review and meta-analysis. The prevalence of MAP antibodies in milk detected by milk-ELISA ranged from 1.1 to 67.7% and the prevalence of MAP DNA in goat milk detected by MAP-specific polymerase chain reaction (PCR) ranged from 1.94 to 37.74%. A meta-analysis indicated a combined MAP infection prevalence of 8.24%, but with high heterogeneity among study findings (I2 = 98.7%). The identification of the MAP in goat milk implies the need for surveillance of the agent in order to prevent economic losses and impact on public health.
Comment
The problem of Johne’s disease in goats has been overlooked for far too long. In Wisconsin, as in many places in the world, the goat industry is growing, particularly for dairy goats. Data from the United States Department of Agriculture, which counts livestock across the United States every 5 years, show just how much Wisconsin dominates the nation's dairy goat industry. In 2017, the most recent year the USDA surveyed producers, the size of Wisconsin's dairy goat herd easily topped the nation at more than 83,000-head. California came in a distant second, with some 43,000 dairy goats, while Iowa, Texas and Missouri rounded out the top five.
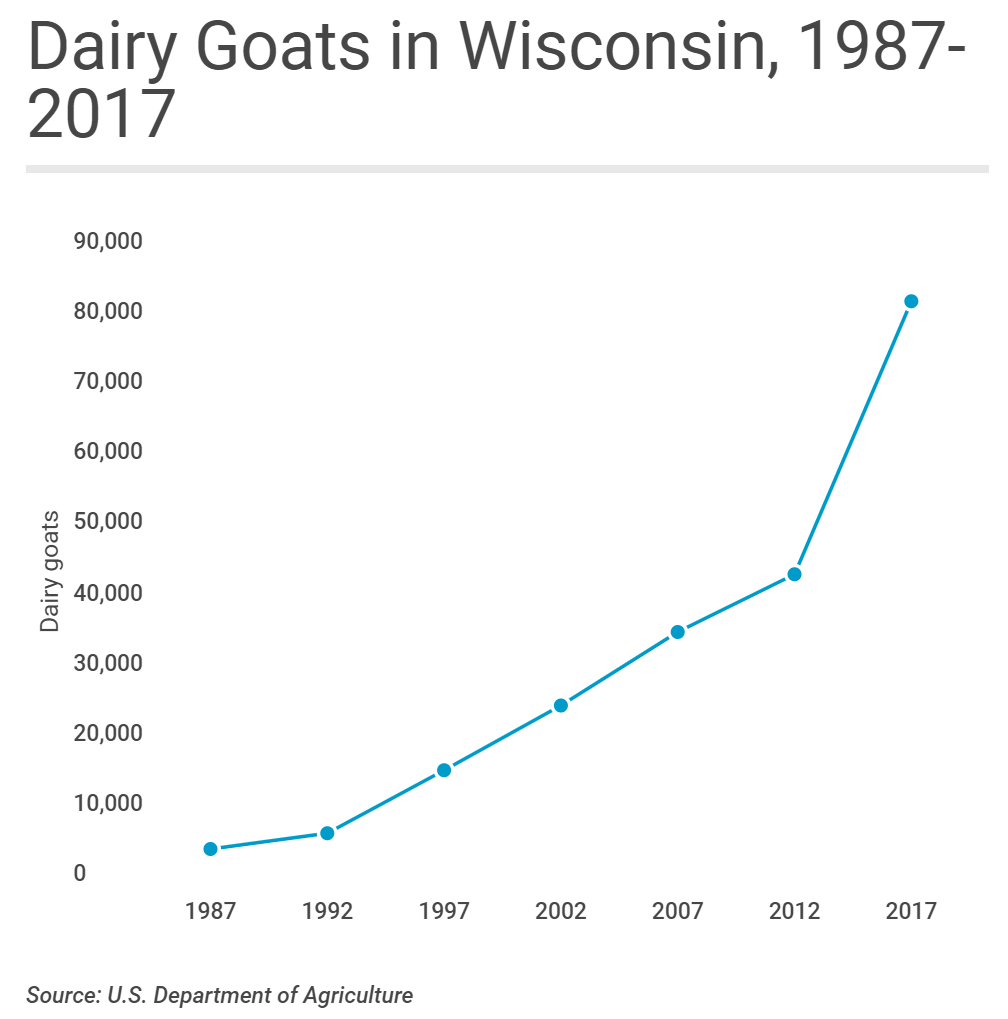
It's not only the sheer size of Wisconsin's dairy goat herd that stands out: The state also leads the nation in the value of sales from dairy goat operations and is the epicenter of national growth in goat dairy. The problem is that rapid goat herd expansion brings with it a high risk of introducing Johne’s disease and once this chronic infection takes root in a herd it becomes a financial drain on the business and a major risk to product sales should MAP become widely recognized as a food-borne zoonotic pathogen.
JD CONTROL ON GRAZING DAIRY FARMS
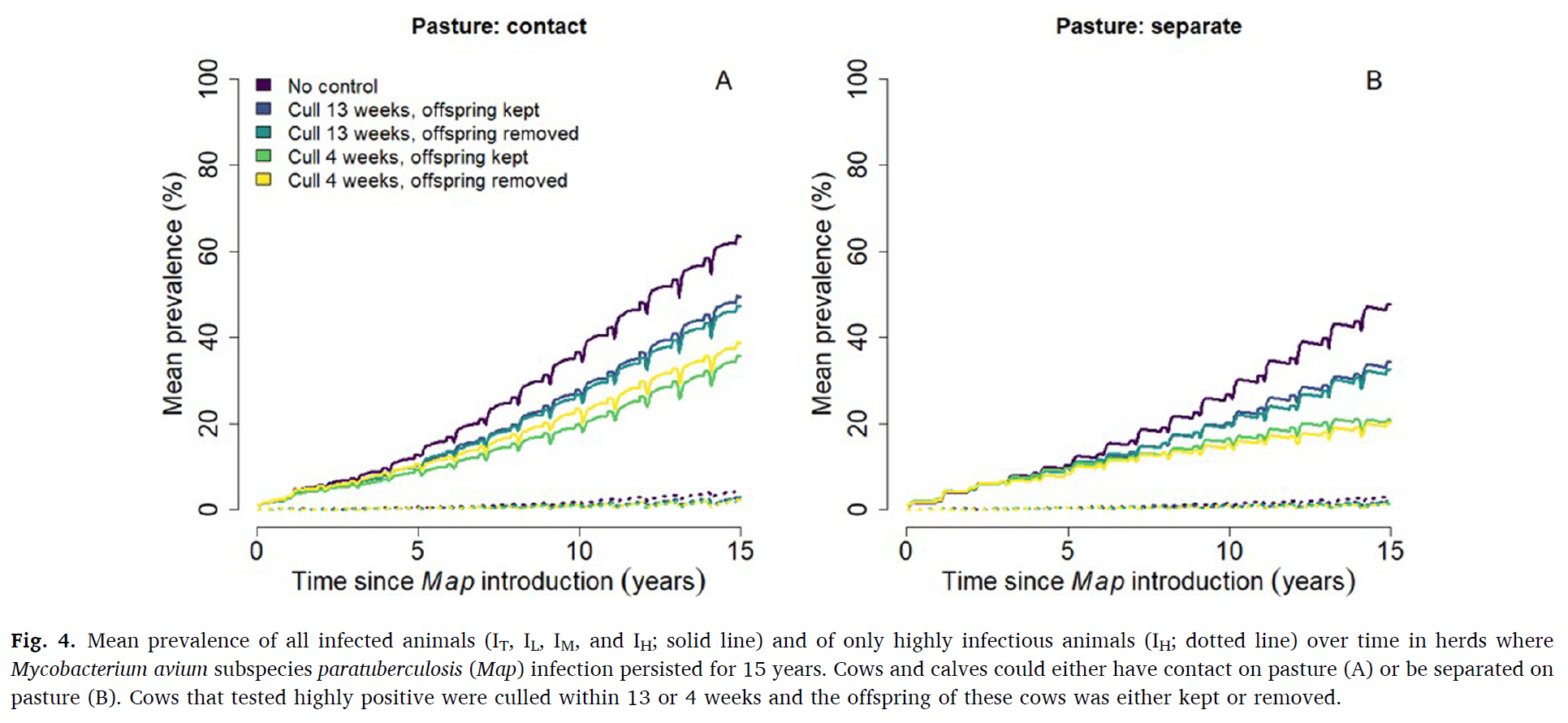
2021-01-21 17:59:21![]() F. Biemans from the Centre for Veterinary Epidemiology and Risk Analysis, UCD School of Veterinary Medicine, University College Dublin, Ireland together with colleagues from INRAE, Oniris, BIOEPAR, Nantes, France and Teagasc, Oak Park, Carlow, Ireland, published a study titled: Modelling transmission and control of Mycobacterium avium subspecies paratuberculosis within Irish dairy herds with compact spring calving. Their article appears in the January 2021 issue of Preventive Veterinary Medicine.
F. Biemans from the Centre for Veterinary Epidemiology and Risk Analysis, UCD School of Veterinary Medicine, University College Dublin, Ireland together with colleagues from INRAE, Oniris, BIOEPAR, Nantes, France and Teagasc, Oak Park, Carlow, Ireland, published a study titled: Modelling transmission and control of Mycobacterium avium subspecies paratuberculosis within Irish dairy herds with compact spring calving. Their article appears in the January 2021 issue of Preventive Veterinary Medicine.
This graphic from their publication shows the spread of Johne's disease in grazing dairy herds with and without appropriate control measures. Annual testing by serum ELISA, prompt culling of the high (strong) ELISA-positive cows and separation of the calf from the cow soon after birth were critically important control measures.
Abstract
Paratuberculosis is a chronic bacterial infection of the intestine in cattle caused by Mycobacterium avium subspecies paratuberculosis (Map). To better understand Map transmission in Irish dairy herds, we adapted the French stochastic individual-based epidemiological simulation model to account for seasonal herd demographics. We investigated the probability of Map persistence over time, the within-herd prevalence over time, and the relative importance of transmission pathways, and assessed the relative effectiveness of test-and-cull control strategies.
We investigated the impact on model outputs of calf separation from cows (calves grazed on pasture adjacent to cows vs. were completely separated from cows) and test-and-cull. Test-and-cull scenarios consisted of highly test-positive cows culled within 13 or 4 weeks after detection, and calf born to highly test-positive cows kept vs removed. We simulated a typical Irish dairy herd with on average 82 lactating cows, 112 animals in total. Each scenario was iterated 1000 times to adjust variation caused by stochasticity. Map was introduced in the fully naive herd through the purchase of a moderately infectious primiparous cow. Infection was considered to persist when at least one infected animal remained in the herd or when Map was present in the environment.
The probability of Map persistence 15 years after introduction ranged between 32.2–42.7% when calves and cows had contact on pasture, and between 18.9–29.4% when calves and cows were separated on pasture. The most effective control strategy was to cull highly test-positive cows within four weeks of detection (absolute 10% lower persistence compared to scenarios without control). Removing the offspring of highly test-positive dams did not affect either Map persistence or within-herd prevalence of Map.
Mean prevalence 15 years after Map introduction was highest (63.5 %) when calves and cows had contact on pasture. Mean prevalence was 15 % lower (absolute decrease) when cows were culled within 13 weeks of a high test-positive result, and 28 % lower when culled within 4 weeks. Around calving, the infection rate was high, with calves being infected in utero or via the general indoor environment (most important transmission routes). For the remainder of the year, the incidence rate was relatively low with most calves being infected on pasture when in contact with cows. Testing and culling was an effective control strategy when it was used prior to the calving period to minimize the number of highly infectious cows present when calves were born.
Comments
Animal husbandry systems heavily influence the options for Johne’s disease control measures. This excellent publication is focus on the type of pastoral or gazing type of dairy herd management prevalent in Ireland. It reinforces the importance of culling the cows with high-positive serum ELISA results and prompt separation of calves from cows after birth. Very interested readers should read the section on model assumptions (section 3.7 on page 8) to judge whether they model fits dairy herd management systems in other their country. In the book Empirical Model-Building and Response Surfaces by Box and Draper (1987) they state: “Essentially, all models are wrong, but some are useful.” I would rank this model as very useful.
Footnote
ELISAs measure the quantity of antibody in the clinical sample which can be either serum (from blood) or milk (for dairy cows). The ELISA reports numerical results called S/P or S/P% values and values above a certain cut-off are classified as positive. However, much more useful information, beyond positive or negative interpretations, can be had when you examine the magnitude of the ELISA result. Animals in the high range, typically with S/P values over 1.0 or S/P% values over 100 are consider “high-positive”, also called “strong-positive”. Multiple studies have shown that this is important information as cows with high-positive ELISA results are the ones most likely to be shedding the most MAP in their feces and milk and most likely to have infected their unborn fetus. Thus, these are the first cows among all of the ELISA-positive animals that should be culled.
JD CONTROL INCREASES DAIRY PROFIT
2021-01-13 01:00:30 Paul Burden and David Hall from the Faculty of Veterinary Medicine, University of Calgary, Canada reported on the variations in the profitability of dairy farms in Victoria, Australia by different levels of engagement in bovine Johne’s disease control. Their publication appears in the January 2021 issue of Preventive Veterinary Medicine. Unfortunately, the article is not open access.
Paul Burden and David Hall from the Faculty of Veterinary Medicine, University of Calgary, Canada reported on the variations in the profitability of dairy farms in Victoria, Australia by different levels of engagement in bovine Johne’s disease control. Their publication appears in the January 2021 issue of Preventive Veterinary Medicine. Unfortunately, the article is not open access.
Abstract
Paratuberculosis or Johne’s disease (JD) prevalence in Australia is low at the cow-level with varying herd-level prevalence. Control strategies incorporating vaccination are limited, suggesting opportunities for changes in regulatory oversight. In order to study this further, we examined the economic benefits of participation in JD control programmes in Australia with and without vaccination as well as knowledge, attitudes, and practices (KAP) relating to JD.
We used an online questionnaire to gather information describing demographics and KAP from 71 Australian dairy farms. Data from fully completed questionnaires from 32 farms in Victoria, Australia combined with cost and revenue data averaged from several years of the Dairy Farm Monitor Project were used to then simulate a larger robust dataset. These production data informed the simulation model to establish farm profitability. A partial farm budget was then developed to estimate the benefits of engaging in JD control activities. Respondents who stated they participated in JD control programmes gained an additional $43.80/cow/year net income (profit) compared to non-participants. Respondents also using a JD vaccine gained an additional $35.84/cow/year over non-users; this represents $10.56/cow/year over and above the average producer in the industry. However, we also noted that there clearly exists a barrier between farmers stated intentions to participate and actual participation in JD control activities.
These significant differences in net income realized by farms using different approaches to JD control (in this case, adoption of vaccination) offer a starting point from which to explore questions of how much farmers would be willing to pay for control activities, why they are willing to pay, and the likelihood of participating. Communication of the benefits of participation needs to improve to bridge this gap between farmers stated intentions and their actions.
Simulation modelling suggests increased profitability from participation in JD control programs and vaccination in Australia. The JD regulatory policies of other countries may benefit from the Australian experience with JD control.
Comments
Vaccination for JD is not an option in many countries of the world, but other Johne’s disease control measures can be done everywhere. Other studies have also shown that JD control improves dairy farm profitability (Roche, Journal of Dairy Science, 2020).
These are the simple steps proven to achieve JD control (see Collins et al. Successful control of Johne’s disease in nine dairy herds: Results of a six-year field trial. J. Dairy Sci, 2010):
- Step #1: have your herd veterinarian do a herd risk assessment to determine which management practices to change in order to limit MAP transmission on the farm.
- Step #2: Implement the necessary management changes with written protocols.
- Step #3: Develop a testing plan with your herd veterinarian coupled to a written “action plan” outlining what will be done with cows based on their JD test results.
JD control is not hard, it simply requires a well-developed plan that is consistently followed for at least 5 years. As the publication by Burden and Hall shows, these actions will significantly improve farm profitability. So, why not do it?
« Previous 1 … 4 5 6 7 8 … 19 Next »